



Why are C-Sections Becoming the Norm?
The Anthropology of Birth shows that things don't have to be this way

Hey Folks,
As you know, I’m always talking about David Graeber. In fact, I’ve made it my mission to read everything he ever published. This will take some time, as he left behind over 5000 pages. I’d guess I’m about halfway through.
Thankfully, I’m not the only one who is doing is. In 2023, a collection of essays was published under the title As If Already Free. The driving force behind it was an Australian anthropologist by the name of Holly High, who was a friend of Graeber’s.
Holly High is a specialist in the anthropology of birth. She did her fieldwork in Laos. As you can imagine, different cultures have different practices and customs surrounding birth. There are so many different cultures with so many practices that there is an entire sub-discipline of anthropology that specializes in this subject.
I have chosen to reprint an essay from As If Already Free which I feel provides an excellent introduction to the anthropology of birth.
I am a man, and not even a parent, so I can’t claim to know too much about birth. But what I do know is that an ever-increasing number of births happen by caesarian section, which doesn’t seem right to me.
According to Statistica:
Global rates are projected to reach 28.5 percent by 2030. Even in 2021, already more babies were born by c-section than vaginally in… Turkey, South Korea, Mexico, Chile, and Poland.
Wow! How crazy is that? For hundreds of millions of people, birth by C-Section is already the norm. How did this happen? And why aren’t people talking about it?
This is a touchy subject, because I’m well-aware that C-sections can be life-saving. Not even the Vatican is against C-sections on principle.
Furthermore, mothers who have had C-sections that may not have been medically-necessary tend not to like it when the subject comes up. They especially don’t like it when it is suggested that there is compelling evidence to suggest that natural births are better for both mother and child. And so the whole subject stays hush-hush.
But C-sections are major surgeries which carry the risk of both short-term and long-term complications. Should they really be the norm?
Anthropology offers us examples that we can compare our own society to. After all, birthing is something common to every single society that has ever existed. And for many decades, it has been known that Western civilization has a particularly dread of childbirth, perhaps owing to our Mythos, in which Eve is cursed with painful labour for eating of the Forbidden Fruit.
Alan Watts, writing in his 1966 masterpiece The Book on Taboo Against Who You Are, had this to say:
[I]t used to be thought that childbirth should be painful, as a punishment for original sin or for having had so much fun conceiving the baby. For God had said to Eve and all her daughters, "In sorrow thou shalt bring forth children." Thus when everyone believed that in having a baby it was a woman's duty to suffer, women did their duty, and many still do. We were much surprised, therefore, to find women in "primitive" societies who could just squat down and give birth while working in the field, bite the umbilical cord, wrap up the baby, and go their way. It wasn't that their women were tougher than ours, but just that they had a different attitude.
For our own gynecologists have recently discovered that many women can be conditioned psychologically for natural and painless childbirth. The pains of labor are renamed "tensions," and the mother-to-be is given preparatory exercises in relaxing to tension and cooperating with it. Birth, they are told, is not a sickness. One goes to a hospital just in case anything should go wrong, though many avant-garde gynecologists will let their patients give birth at home.
When I read that, I was quite surprised. But then I thought about it. Women have been giving birth for hundreds of thousands of years. Clearly, they were able to get the job done long before the advent of modern medicine.
Also, I’m well-aware of the power of suggestion. In myriad ways, we create reality with our beliefs. Could the painfulness of childbirth be worsened by cultural expectations?
THE WAR ON WISE WOMEN AND THE RISE OF THE MALE DOCTOR
Furthermore, I’ve read quite extensively about the European witch hunts and know that the Cult of the Male Doctor arose as a result of a war on women’s reproductive autonomy.
Very briefly, the drastic decline in Europe’s population after the Black Death led to a scarcity of peasant labourers, which increased their relative bargaining power. Feudal lords now competed for workers, and peasants took advantage of their new power to demand better higher wages and working conditions.
The Powers That Shouldn’t Be responded by launching a class. Because contraception, abortion, and midwifery were everywhere the domain of “wise women”, a campaign to vilify those women as witches was launched. The goal was to increase the number of peasant labourers by eliminating the practices of contraception and abortion. It also served to forestall the risk of peasant revolt by turning men against women. Then, as now, the essence of statecraft was “divide and conquer”.
The best introduction to this subject is the classic pamphlet Witches, Midwives, and Nurses by Barbara Ehrenreich and Deirdre English.

(Disclaimer - Please note that this time period is incredibly complicated and a single pamphlet cannot possibly do justice to all of the many factors that coalesced in the witch hunts.)
Following a campaign of terror against traditional medicine, female midwives were replaced by male doctors, and the era of the Cult of the Male Doctor began. Female nurses still did the lion’s share of the work when it came to providing healthcare, but they were now subordinated to the authority of the male doctor.
To this day, female nurses defer unquestioningly to the supposedly superior knowledge of doctors, who are still mostly male. The medical profession suffers from a deeply ingrained sexism, yet it is hard for many to see, due to the fact that female nurses are such willing participants. The oppressive nature of Western medicine, which has long privileged male authority over female wisdom, persists even as more and more women become doctors.
If you are interested in this subject, I would highly recommend reading Influence by behavioural psychologist Robert Cialdini, who examines the doctor-nurse dynamic in his study of the psychological principle of Authority. In it, he shows the extent to which nurses are conditioned to obey doctors, which is quite disturbing. There is little doubt in my mind that healthcare would improve if nurses were more empowered.
When male doctors took control of childbirth, women were instructed to lie down on a bed, rather than squatting or walking on all fours.
It seems probable that this led to increased pain in childbirth. When giving birth, why wouldn’t you want gravity on your side? Squatting seems a no-brainer.
My theory is that male doctors didn’t want to be reminded of the animality of birth, and thus forced women to adapt themselves to their ideas of propriety.
Perhaps on some level they thought it right and proper that women should suffer intense pain when giving birth. After all, wasn’t that was the Bible said should happen?
All these centuries later, we are still dealing with the consequences of the Witch Hunts. There is no way that a man could possibly understand the experience of childbirth as much as a woman who has actually gone through it. Midwifery should be the domain of women, not men.
A CONTRIBUTION TO THE EMERGING CRITIQUE OF ANTI-NATALISM
Anyway, these are some of my thoughts, which I offer as a contribution to the political reorientation currently occurring in feminist/post-feminist discourse.
Lately, I have offered many harsh critiques of what I call “Fourth-Wave Feminism”, which is better known as woke feminism, transfeminism, or intersectional feminism.
Indeed, the feminism brand has become so unpopular that even hardcore feminists such as Meghan Murphy have distanced themselves the label. More recently, Meghan Murphy has embraced the label TERF, which she long rejected, and it is increasingly clear that radical feminists have won the debate over trans ideology. That said, by no means does that mean that we’re back in the second wave of feminism. There’s no going backwards.
My main critique of fourth-wave feminism is that it is dominated by childless women, who cannot claim to represent mothers. As Terri Strange and Mary Harrington have pointed out, feminism has had an implicit anti-natalist bias for at least a decade.
One of the characteristics of the emerging Fifth Wave of Feminism is a rejection of anti-natalism.
Obviously, feminism is all about bodily autonomy, so women should not be pressured to have children if they do not wish to, but it should be equally obvious that motherhood is an integral part of womanhood. Worldwide, something like 80% of women will become mothers in their lives. Motherhood is hardly tangential to feminism.
If you ask me, the best book written by a woman in the past 25 years is Mothers and Others by Sarah Hrdy, which has revolutionized evolutionary theory by introducing the concept of “cooperative breeding”. Somehow, this book seems to have escaped the notice of most feminists.

Anyway, there is a lot that can be learned about motherhood from the anthropological record, and one of the most surprising things is that the pain of childbirth seems to be partly determined by cultural expectations.
This is not to say that the pain of labour is not real, but it is to say that Western Civilization might fear childbirth more than it should. Our minds are powerful, and we create reality with our beliefs.
What are the limits of this? We won’t know unless we study childbirth in other cultures. Hence, the anthropology of birth.
Lastly, yes I know that I’m a man and my perspective is limited by the fact that there are parts of the female experience that I cannot understand. I get it. Please forgive me if you feel judged by my words, such is not my intention. My goal is to start a conversation. I consider it my job to say things that need to be said, but which other people aren’t willing to say. And there is no doubt that C-sections are a taboo subject.
My message for the world is basically things don’t have to be this way. The anthropology of birth provides one extremely powerful example.
Enjoy!
BIRTHING POSSIBILITIES
by Holly High, excerpted from As If Already Free
There is a moment in September 2020 that is preserved with strange clarity in my memory: I was sitting on the brown leather sofa at home, then in the southern highlands south of Sydney, when my phone buzzed and the screen lit up. “I just wondered if you saw that,” a former student had texted, with a link to a news story. When I read the article, I had a ludicrous moment of denial. “Is this a hoax?” I shot back, slightly irritated. But my student gently pointed out that David Graeber’s agent had confirmed it: Graeber was dead.
During those September days, I had been preoccupied with online teaching, beaming out lectures and tutorials from a home-office (jammed in awkwardly behind a piano in the lounge room). The pandemic was biting deep across the world, and even as teaching expanded into the online space, still my world felt reduced. COVID-19 had come to us in Australia so soon after our Black Summer, when the southeast eucalypt forests burned as they never had before. For months, with every breath, we grimly took in the incineration of millions of wild animals. Graeber once described himself as a “professional optimist.” He never ignored violence or injustice in his work, yet he still always saw great possibilities for we humans. I kept wondering what he would have made of these days of fire and plague. What paths out? For weeks the news of his death left me in tears at odd moments. I counted myself among David’s friends, but we were not particularly close. It wasn’t clear to me what, exactly, I was grieving. So, between teaching, I wrote.
My lectures and tutorials that September were for first-year students: I was introducing them to the discipline—to this “passion for difference” that I believe to be anthropology’s gift—by discussing something we all have in common: being born. I invited students to interview their mothers or care providers about the circumstances of the students’ own births. I had been trying to teach them that listening to stories is important; that cultural context, difference, and change do exist and can be understood; and that, though cultural messaging, and norms and structures, and natures necessarily shape us, we are, nonetheless, capable of freedom.
In those first weeks after David’s death, I realized I wanted to write that his anthropology opened possibilities for thinking anew about birth. But my first drafts were angry. I quarreled with him for not mentioning this and not theorizing that. He never directly engaged with the anthropology of birth. Perhaps I was just passing through another stage of grief: the angry one. Or perhaps it is just that, when we value something, when it becomes a token of value for us (to use Graeber’s phrasing from his 2001 book False Coins of Our Own Dreams), on some level we always know that we see in it something that is not there. And that something we value, that hidden dimension—which we so often misperceive as the power of valuable objects—Graeber suggested, is in fact our own capacity to act. That has been my experience of grief, too. The force of it—the disbelief, anger, and loss—is disorientating, but resolution can be found when the lost is understood as also somehow kept.
This chapter is the result of thinking about the anthropology of birth alongside David Graeber’s anthropology. Although not usually thought of together, there is a significant kinship: both can be read as examples of activist anthropology and show the potentials (and pitfalls) of an anthropology that chooses to rebel. I argue that these two threads of the discipline can be joined in ways productive for both.
II
As a child of my time, I did not think particularly deeply about birth until the prospect of my own labor was on the horizon. In preparation for the birth, I asked my grandmother, then in her eighties, what to expect. It was a family gathering in June 2013. We were sitting side by side at the long, polished dining table that fills almost the entire dining room of a cedar-wood farmhouse outside a town in the Great Dividing Range of New South Wales, where we’d spent many Christmas lunches. We were just a few kilometers from where she had raised her five children, at first in a shed on the land her husband had been granted after he returned from World War II. Pa never spoke about the war, except to severely ban us from pointing a gun, even a toy one, at anyone, ever. When I was an adult, I realized the land we were on had been taken from Indigenous people. My mother said that some of those first owners lived in a camp on the country there and worked odd jobs as Pa and Joan’s sheep farm was established. I do know that one of the nurses that cared for Joan in her last days was a descendant of the people that had lived in that camp, but that is all I know. That is another conversation I never had with Joan.
When Joan had her first child, she told me, her father would come to visit from town. One-way, the journey took a full day by horse and cart, stopping and stepping down every few kilometers to open a gate and shut it behind him. It was not until her fourth child was born that the home they had been building—a pink, architect-designed, flat-roofed, 1950s beauty, incongruously placed on a dusty rise with a far-sighted outlook across the paddocks—was ready for the family to live in. They also acquired a car, and Joan and Pa would make the long drive into town jubilantly singing “Qué será, será” to the children, to distract them, my mother thought, or perhaps simply from the infectious optimism that seemed to saturate the mood of 1950s Australia. Pa died from Parkinson’s Disease when I was a child. Much later, I learned that his children believed that this was likely due to his exposure to chemicals during his work on the farm. But no one spoke of this to me at the time. At his funeral, we heard that, in his dying days, he said of his life: “I married the woman I loved and put a dam in every paddock.”
I was leaning toward Joan across my new and strange belly, and her smile seemed to say: no judgment that your pregnancy preceded any sort of marriage or even a plan for one. No bad words. No painful memories. Around us, the hubbub of her children, her children’s children, and their partners: the joy of the crowd seemed to set a limit on what we could say. When I asked what birth was like, she laughed and told me not to think too much about it: “The doctor will give you something and you will go to sleep. When you wake up, there will be a baby. The doctor will do it all for you.” I didn’t press her. Not long after, and before my first child was born, Joan died.
III
Anthropology, my profession, is my other family. By reading and (much more rarely) meeting anthropologists whose work I admire, I have found people willing to have the kind of conversations that might be too difficult in one’s real family, but who still have that family-like ability to shape who you are. In pregnancy, I dug out old readings given to me when I was an undergraduate studying anthropology at the Australian National University. I remembered Robbie Davis-Floyd’s 1994 article on birth in the United States: I had also given that article to my sister when she was pregnant before me, but it had not clicked for her. For me, though, it provided a searing warning about the implications of the “technocratic” turn taken by biomedical approaches to birth in the twentieth century. Davis-Floyd used Arnold Van Gennep’s 1909 concept of rites of passage to interpret the otherwise unnecessary interventions that riddle hospital births, like the use of wheelchairs, monitors, and bizarrely designed delivery beds. Davis-Floyd understood these as symbolic, part of a deeply sexist set of rituals that repeated the cultural messaging that women are faulty birthing machines and that technology provides the only sure means of regenerating life. According to Van Gennep’s formulation, a rite of passage is a series of rituals during which a person who is moving from one status to another undergoes first a period of separation from her previous everyday life, then a liminal stage—a threshold, neither here nor there—and finally a period of reintegration into her new role. Van Gennep included birth as a key rite of passage in his original study, arguing that both mother and child move from one status to another, as evidenced through symbols such as eating prohibitions and bans on work or religious activities. Van Gennep’s interpretation of rites of passage was quite conservative, though, inasmuch as he did not seek out the seeds of cultural change in his study, or even really consider the possibility of social change at all. Instead, his emphasis was on how these rites effectively reproduce existing social roles among new initiands. Victor Turner later reinterpreted the liminal stage as a potentially creative space. Turner thought that the liminal stage was a time where the old certainties of life-as-it-had-been become loosened and uncertain, but when at the same time the new certainties of life-as-it-shall-now-be for the initiand in their new status have not yet coalesced. It was true, he acknowledged, that one finds all kinds of conservative symbolism in rites of passage, and that these can predispose initiands to a repetition of the established social order. But one also finds inversions of these, and also suggestions of unorthodox values and possibilities. Turner imagined the liminal stage as a kind of social limbo where one could glimpse all kinds of symbols, including the seeds of other ways of being. As I would later go on to tell my students, we will each pass through rites of passage whether we like it or not and whether we know it or not. These occur when we pass from one status to another, as when a school student becomes a university student, for instance, or when a child is born, or at retirement, and so on. If we can recognize a rite of passage for what it is, though, we do have some measure of freedom: a freedom to accept, or work with, or jam the symbols we live in these times of our lives.
Thinking within this tradition, I sought out the rituals of separation, liminality, and reintegration evident around me in pregnancy. I observed the people nearest to me responding with gifts for the baby. Although I did not have a baby shower, nonetheless it seemed plain that, for many people, preparing for a birth involves the acquisition of goods. Succumbing to this pressure somewhat, my partner and I made a trip to a gigantic baby-goods store and wandered the aisles, not quite convinced of the necessity of any of it but seemingly not quite able to rid ourselves of the sense that at least some gesture was required. We ended up buying an elaborate contraption for the baby to sleep in: I was still unaware, at that time, that infant sleep is another heavily ritualized field of worry and consumerism in our milieu. These revelations were still to come.
Another ritualized element evident in my first pregnancy was worry. I tracked my budding pregnancy through daily urine strip tests, seeking confirmation through the ever-darkening purple line of whether the pregnancy was real or not. On my first consultation with a doctor about the pregnancy, I was told explicitly to worry. “It is a very inefficient process,” the GP said, meaning that I would likely miscarry. She prescribed me low-dose aspirin. After a conversation with my partner, I decided not to take it. The GP prescribed an ultrasound at nine weeks to assess if the pregnancy even had a heartbeat. It did. The ultrasound technician seemed as puzzled as I was as to why the ultrasound had been necessary. At twelve weeks, my doctor prescribed a nuchal translucency test to assess risk for Down’s syndrome. This again involved an ultrasound. It was quite pleasurable seeing the outline of the little future-person in my belly, but the technician went quiet and left the room to fetch the obstetrician. On arrival, with great gravity, the obstetrician reported that my son’s nasal bone did not look normal. In words that are branded into my memory, she said “If you were Asian, we would not be worried. But as you are Caucasian, we would expect a different nose.”
On that basis, which to me seemed entirely spurious, along with statistical formulas (largely based on my age), I was given a result of 1 in 17. This represented their assessment of the chance my son had Down’s. The obstetrician requested that I consent to an invasive procedure that had a 1 in 100 chance of aborting the fetus. All my instincts told me not to do the procedure. But my partner and the obstetrician persuaded me. With such forceful cultural messaging prodding me into seeing my pregnancy through the eyes of science, my pregnancy looked risky, unsure, full of worry. I had the test. It revealed that the obstetrician’s fear had been misplaced.
To this point, my pregnancy conformed to the kind of rites of passage Robbie Davis-Floyd described: the messages were that women’s bodies are faulty and inadequate for efficient birthing, that my own ability to reproduce was very questionable in itself: for a successful outcome, I ought to rely on medical technology. The view of my pregnancy afforded by medical technology (such as the pregnancy test strips and the ultrasound images) was surer than my own, and to be a mother at all, and especially to be a good mother, I ought to defer to that way of seeing my pregnancy.
Yet this was not the whole story. The debacle with the nuchal translucency test was a wake-up call for us. We hired a private midwife, Sheryl, and started planning a home birth. Unfortunately, due to an early rupture of membranes with no labor at 36 weeks (which I will forever link to the unnecessary invasive procedure inflicted by the obstetrician during the nuchal translucency test), I birthed in hospital under induction at 37 weeks. Induction is notorious for sparking a “cascade of intervention” because the synthetic oxytocin used does not cross the blood-brain barrier, meaning that contractions occur without the usual accompanying benefits of feel-good hormones. The contractions can easily build up too fast and too hard, creating unbearable pain and pressure on the baby. Knowing these risks, we opted for induction anyway. The hospital midwife attached a monitor to my belly to track the baby’s heart rate and to look for signs of distress. I took it off. I requested a bath. The hospital midwife left to ask the obstetrician on duty if it was permissible for a woman who was being induced to birth in a bath. Sheryl went to fetch some warm water to top up the bath, in a quiet defiance that this question had even been raised. While they were both out of the room, I entered the bath and experienced a “fetus ejection reflex”: the baby was born in a single spasm.
It was a moment of great clarity. I want to say that it felt powerful, but not in the sense of being in control: I was completely out of control. My normal self was gone. I was overwhelmed. But something of me was in control: something not me exactly, but of me. It was a part of myself I had not encountered so consciously before. I felt that a me much more powerful than my conscious self had snatched birth back from the grips of the less-than-perfect circumstances around us and done it simply, gloriously, and rebelliously without asking anyone’s permission. Sheryl came back in just after the baby’s head was born: she was so sure that we were hours away from crowning that she almost tipped a steaming bucket of boiling water right in, but luckily saw the emerging baby just in time. Instead, she instructed us on how to pass the baby safely through the water, and then snapped a photo of the three of us, my partner, our baby, and me, jubilant. It was a very affirming note on which to begin my journey as a mother, and also for my partner who was commencing his new role as a father.
It seems to me that this is the key point about liminality. It is true that rites of passage can imprint new initiands with conservative meanings. All the rituals of birth that Robbie Davis-Floyd described in her 1994 article about hospital birth happened to me: the almost obsessive concerns with dilation, the bright lights, and the monitoring devices all repeating the cultural messaging that my body was a faulty birthing machine and could only be made to work through medical technology. But birth is not always reducible to the rituals constructed around it. Even in conditions of intense ritualization, such as a hospital birth, one finds seeds of other meanings
IV
The first birth I remember attending was on an island in the Mekong River where I lived for 16 months for ethnographic fieldwork in 2002 and 2003. The village was a string of 50-odd houses on stilts, spaced out between gardens, bamboo, and coconut palms along the riverbank. The houses, which were made of teak and bamboo, faced the river, and backed onto rice fields. A gilt Buddhist temple gleamed on the higher patch of ground in the village center.
One day, I noticed a house downstream preparing a screened-off area under the house: an area, my hosts told me, for the coming birth. I walked by, curious and ever the diligent fieldworker, but too shy to intrude on what I assumed was a private event. I was pleased and surprised, then, when a lean young man, perspiring from the heat and a long walk through the dark of the evening, came to my house to invite me. He was inviting every household, using a headlamp to follow the footpaths between houses and across rice fields. Birth was one of the occasions (along with deaths, severe illnesses, marriages, and feeding the dead) that required at least one member of each house to attend for an all-night vigil. By the time I got there, though, the birth itself was over. While the woman who had just birthed rested in the screened-off space under the house drinking hot liquids and “toasting” over hot coals (really, just sitting close by or over the coals, in a ritual seclusion where heat is thought to help the body dry and close after birth), we congregated upstairs listening to music, dancing, drinking alcohol, and eating delicious morsels.
It is compulsory at such events that men gamble with playing cards. Gambling is usually illegal in Laos, but these rules are informally suspended at birth parties. Events like these are so expected that, in the case that a birth is not accompanied by a birth party with extensive gambling, it is generally understood to be an indication of the severe poverty and marginalization of that family. In Luang Prabang, where people are much more prosperous than in the rural village where I conducted fieldwork, these parties can go on for a month, with the regularity and length of any given guest’s involvement in the party taken as a sign of their closeness to the couple who had birthed.
In my field site, these events were typically referred to as wiak (L: labor, in the sense of work). Labor, in the sense of birth itself, is instead referred to by the direct word cep (L: pain). If birth labor in Australia implies the labor of faulty bodies at producing a product (much like a factory worker might labor on a production line), in Laos, the meaning of birth labor is the sociability around the birthing woman. Birth labor here is the work of revelry, the effort it takes to suspend everyday rules, and the contributions we all made by simply being there, adding to the creative, out-of-the-ordinary spark generated by gatherings. Birth was a carnival. No wonder so many women prefer to birth at home in Laos.
Since having my own children, I have paid more attention to birth in Laos. One of the characteristics of the births that I have followed in the southern provinces of Champassak and Sekong is that, even though most women broadly respect medical science, in general, the preference and practice is to birth outside of medical facilities, even when doing so means that medical assistance may be too distant to access in the case of an emergency. In explaining this, women cite lack of transport, “shyness” of (and sometimes outright shaming by) medical staff, the convenience of a village birth for the friends and family who may wish to attend, and cost (even though mother-and-child health care is free in Laos). I have seen women plan a hospital birth, but when the time came, they ended up birthing in the village, saying that it never felt like the right time to go. Women also very frequently say that if they are not sick, they do not see the need for medical care. Many do not see pregnancy and birth as an illness, and when I probed them on this, I heard about the reassuring messages they received from the people closest to them. Many come to their first pregnancies having observed dozens of births firsthand: people growing up in a Laos village have often had ample opportunities to observe the births that take place there, or at least attend directly afterwards, as I mostly did. My own observation is that children are the most numerous of the attendees at a village birth in Laos. The children in Laos I have known did not grow up in ignorance and fear of birth.
In a Laos village, much cultural messaging affirms that birth is nothing to fear. And indeed, the births I knew of seemed to be usually trouble-free and over in an hour or two. All this, despite statistics suggesting that Laos has the highest maternal death rate in Southeast Asia. By contrast, in Australia the cultural messaging around birth seemed to dwell on its uncertainties (what to expect?) and dangers. The few births I had close knowledge of before having my own children seemed drawn-out and vexed, typically beset by high drama, angst, and epic time scales (by Lao standards at least). This, despite maternal deaths being considered, statistically speaking, rare in Australia. Clearly, these statistics—while no doubt indicating something true about birth—failed to capture something else: how birth is imagined in each context.
V
When I was pregnant for the second time, I interviewed my mother about my own birth. In a telephone call I made from my back veranda, while surrounded by piles of laundry in various stages of hanging, drying, and folding, I asked and she answered. We were sometimes halting, some- times fluent, feeling our way around shame, reserve, and anger. I was her second child. Her first birth was in a hospital, where she had experienced what birth activists now call “obstetric violence”: without her consent, she was given an unnecessary and painful episiotomy while her husband was forced to remain outside. When the pair were pregnant for a second time, she again enrolled at a hospital and went for regular check-ups. What she didn’t tell these medical providers was that she had also hired two “healers,” Carole and Norman, who agreed to attend her in birthing at home. Despite some misgivings about Carole and Norman’s commitment to homeopathy and an anti-vaccination stance, she did birth at home. During the labor, they offered her drops of Rescue Remedy on her tongue and “Tibetan pills”—hand-rolled by lamas—said to open her birth canal. This was the mid-1970s and my parents were then living on an MO (a multiple occupancy, a “commune,” if you will) in the hinterlands around Nimbin, the center of Australia’s counterculture. My father told me that, in the movement in those days, birthing at home was considered a key aspect of building community, a key affirmation of countercultural values. After I was born, my mother met weekly with other women in a “Pregnancy, birth and beyond” group in Nimbin. I grew up with the photographs taken at my own birth: my mother prone on a bed, sunlight streaming in on her glasses and her long blonde hair, me a bloody blob just visible between her legs, and around the bed, people unknown to me looking on. These were nothing like the stylized birth photography so common today. These were raw.
During our interview, some of the pauses in my mother’s retelling seemed to be around shame, fear, and anger. Looking back now, she wondered: Had it been safe? Had she taken too many risks? When I was a child, she had often said that I was born with the umbilical cord around my neck, as if she was haunted by an horrific “what if” scenario of strangulation at birth. Birth specialists today no longer speak of the umbilical cord as potentially life-threatening for infants at birth, although the idea of tangled umbilical cords did have some currency in the 1980s. The idea of the umbilical cord—that link between us— choking me before my first breath seemed to have come to stand for all the reservations and compromises my mother had faced in planning her home birth in circumstances where there was so little in the way of medical support available for it, and a nightmare possibility that haunted those choices.
Nevertheless, I grew up telling people that I was born at home: I was a home birth. I had some childish sense that this difference was special, a bit like being left-handed. It was only as an adult that I realized that my story had been wrong. In fact, the birth was what people these days call a “free birth”: a birth that is planned and intended to occur with no attendance by anyone qualified in biomedicine. A home birth, by contrast, is a birth that takes place at a woman’s home while attended by a qualified midwife or equivalent. But such births were not an option in 1970s New South Wales. If they are an option today, it is due in large part to women like my mother. Women who rebelled.
VI
My mother continued in birth activism. When I was in high school, she was working to connect local midwives to a home birth group. The numbers were always small, the bureaucratic challenges almost over-whelming, the threat of deregistration always lurking for midwives who supported home birth. David Graeber once wrote, “to live as a rebel—in the constant awareness of the possibilities of revolutionary transformation, and amongst those who dream of it—is surely the best way one can live.” But what is the price of rebellion? When I first met David, we were both new to the United Kingdom.
In our first email exchanges, he seemed cagey, suspicious, and quickly told me that he was in “intellectual exile,” after being denied a place in the United States Ivy League because of his activism. In the introduction to this volume, Josh Reno and I argue that, at least from Graeber’s perspective, at least ten years of his career was spent in a kind of “wilderness,” where he felt that his contributions to anthropol- ogy were undervalued, but also that his activism had cost him his career and his personal happiness. Graeber’s activist sensibilities may have been a large part of the impact his work had beyond the discipline, but they also drove a wedge between him and the mainstream of anthropology, at least from his perspective, and at least for a period.
The same can be said for the activist streak in the anthropology of birth. For instance, my midwives and my mother had all read the works of anthropologist and childbirth educator Sheila Kitzinger, while I, a trained anthropologist, had not registered her work until I was pregnant myself. I am confident I am not alone in this ignorance, at least among my own generation of anthropologists: I ran pop surveys at the slow workshop behind this edited collection (discussed in the Preface to this volume) and during my talks to anthropology audiences about this chapter, and I found that by far the overwhelming majority of anthropologists also did not recognize her name. Like others in my generation, I had been schooled in the anthropology of reproduction as a matter of course, but I was less familiar with the distinction between that larger field and the smaller subfield of the anthropology of birth. The anthropology of birth pre-dates the anthropology of reproduction, and although it was later folded into the anthropology of reproduction, this subfield has a stronger tradition of activism, opening possibilities for birthing women. Brigitte Jordan, Sheila Kitzinger, and Robbie Davis-Floyd are considered the founders of the anthropology of birth. Kitzinger alone wrote over 30 books over a span of 40 years. Her obituary in The Guardian suggests that “She could reasonably be said to have done more than anyone else to change attitudes to childbirth in the past 50 years.” Kitzinger’s 2004 book The New Experience of Childbirth sold over a million copies. Among her hundreds of articles are hard-to- ignore titles like her 2001 “The Great Childbirth Blackmail” and the 2006 “Birth as Rape: There Must Be an End to ‘Just in Case’ Obstetrics.”

Cross-cultural comparisons have long been a part of the anthropologies of birth and midwifery. Brigitte Jordan’s Birth in Four Cultures: A Crosscultural Investigation of Childbirth in Yucatan, Holland, Sweden, and the United States, first published in 1978, is widely considered to be the founding text of both fields. Carol McCormack’s 1982 Ethnography of Fertility and Birth also aimed at gathering culturally diverse details of lived experiences with the aim of improving maternal health care. Later, Sheila Kitzinger’s Ourselves as Mothers: The Universal Experience of Motherhood attempted a survey of the world’s cultures of birth explicitly as a means of prompting readers to reflect critically on their own rituals and practices. Perhaps one reason Kitzinger’s work received less attention in the discipline, despite her broad popular appeal, was the way she used the ethnographic record. While Kitzinger described herself as an anthropolo- gist and often commented on her fieldwork in Jamaica, her texts arguably were the most alive when critically describing experiences in her own society. Her cross-cultural comparisons, by contrast, were often broad- brush indications of “pre-industrial” societies as a foil to the more familiar “technological” societies. At one point she commented that, “When I started studying social anthropology I soon realized that social systems are all about male power and the way in which men organize themselves so as to own, exploit, and exchange women and children.” This is a reading of the ethnographic record for inevitabilities, not possibilities. While this view has held significant currency in mainstream feminist anthropology, there were always other, and more hopeful, readings of the ethnographic record, such as Eleanor Burke Leacock’s 1981 Myths of Male Dominance.

In the mainstream anthropology of the 1980s and 1990s, students learned about the dangers of fast and loose comparisons and universalizing statements. In place of contrasting cultures and statements about humanity as a whole, students learned of insidiously pervasive biopower and the “-scapes” of a globalization that were taken to be inevitable fact. Influential social theory devoted itself to describing its “flows” or, perhaps, the moments of “agency” found in personal consumption. George Stocking, a historian of anthropology, described a moment in the Chicago anthropology department in the 1980s–1990s in an attempt to capture this significant shift in the mood of the discipline. A world map had long hung in the Chicago department, proudly displaying colored flags pinned over each of the field sites studied by students and staff, and photographs snapped of researchers in the field. These showed exotic-looking people, mostly dark-skinned, and their mostly pale ethnographers, as if to indicate that anthropology was the discipline that made comparison between “them”, and between “them and us”, possible. But by the end of the 1980s, this display no longer seemed proud or innocent, with one student commenting that it effectively symbolized how: “the sun never sets on the colonial empire of Chicago anthropology.” While early to mid-twentieth-century anthropology produced many grand syntheses and empirical generalizations, now many anthropologists devoted them- selves to understanding local people on their own terms, which in practice meant years of language learning and “being there” in often small or niche field sites. These committed fieldworkers barely dared to make regional comparisons, let alone global syntheses. In this context, magpie collections of examples drawn from different cultures, such as those assembled by Kitzinger, came to strike many anthropologists as naïvely decontextu- alizing at best, or at worst as participating in an imperialist worldview.
Graeber, who went through his PhD training in the Chicago department and period that Stocking described, agreed with the need to avoid comparisons that subordinated local particularities to universal inevitabilities, but he wanted to do so in a way that maintained the link between ethnographic comparison and activism. In one of his earliest books, he pointed out that:
While anthropologists are effectively sitting on a vast archive of human experience, of social and political experiments no one really knows about, that very body of comparative ethnography is seen [within the discipline] as something shameful … it is treated not as the common heritage of humankind, but as our dirty little secret. He noted wryly that keeping the ethnographic record as anthropology’s dirty little secret was still a way of keeping the ethnographic record, keeping it to ourselves, and refusing to share it with the wider world.
These criticisms are, of course, simplifications: Graeber acknowledged as much. But in articulating the situation so simply, he put into words an unease that many anthropologists had felt about the de-politicizing effects of the turn to endless local contextualization. In so doing, he defended the possibility of intentional social change, even revolution, and the role of anthropology in that. And in doing so, he inspired the generation of anthropologists that would come after him, my generation.
Graeber would go on not only to defiantly practice comparative ethnography, but also to put it to work in answering questions provoked by his activism. In the Afterword to the 2014 edition of his bestselling Debt: The First 5000 Years, he noted that he had deliberately set out to write a sprawling, scholarly work of the kind that was distinctly out of fashion when he commenced that project. His book—while unabashedly schol- arly and presenting complex ethnographic material—spoke clearly to popular concerns, such as anti-globalization, Occupy, and the 2007–8 financial crisis.
VII
Kitzinger’s work arguably provides an even plainer example of the activist potentials of comparative anthropology. Many of those who celebrated her life after her death in 2015 argued that the revolution that Kitzinger fought for was won in her lifetime: humanistic changes in childbirth were achieved in many countries. Her anthropology touched millions of lives. I birthed in a post-Kitzinger world, in a setting shaped significantly by the kind of care Kitzinger championed. My second birth was a home birth, a true home birth, attended by a qualified midwife, Rachele.
The build-up of contractions was slow. Five days out from the due date, there was some cramping, blood, and gushes. Rachele encouraged us to go about life as usual, so we did. Without my noticing it very much at first, I found that these cramps became the tempo of my life: I could stand up easily, but I’d wait for the cramp to finish first. If I lingered by the warmth of the oven, it was to ease the cramp that was passing then. If I spoke, it was because there was no cramp, and if I hummed softly, it was because there was. Mostly I was my normal self, but when the pain came, I paused, became more inward.
Things became more intense at about nine o’clock on the night before our due date. Now when the pain came it would take all of my attention. For what seemed like hours, I leaned on a chair in the dark of my bedroom in solitude, feeling waves build and subside. It was hard work, but it felt pleasant and possible. I loved the TENS (Transcutaneous Electrical Nerve Stimulation) machine: a non-invasive, drug-free method of pain relief. Who knows if these things really work? Part of the pleasure of it no doubt was the mindless, repetitive action of turning it up at the start of each contraction and down at the end, both done with the press of a button. It marked the passing of each contraction and put me in charge (it was my finger on the button!). I enjoyed the breaks between the contractions. I was entering what philosopher Orli Dahan has tentatively called “birth consciousness,” which she defines as “an altered state of focus and retreat” which may feel spaceless, timeless, and nonverbal. Sometimes when my partner came to check on me, I could not muster any words. At one point I gathered myself especially so I could explain to him that if I was not speaking, it wasn’t because there was any problem. I was just too ecstatic. I asked him if he’d ever felt so high that he imagined entire conversations with people but when he went to speak, realized that none of it mattered because it was all beyond words? Well, that was how I felt at the time. Ridiculously happy, truly gone.
Through all this I heard Gadsby (my firstborn) crying: it was hours past his bedtime. From the bedroom I commanded: “Bring him here.” Gadsby curled up in my arms as I sat on the floor in the candlelight, humming through contractions while rocking him. He looked up at me, curious but mostly sleepy. I relished letting the deliciousness of his gentle, drowsy presence, his blonde curls and angelic face, sink in, aware that this would be the last time for a while that it would be just the two of us. Gadsby slept. I laid him on the bed and rested next to him for a while. The contractions ceased, and I must have fallen asleep or into some kind of doze. Perhaps 20 minutes passed. My partner came in to check, and I got up in that way you do when you are half asleep and for some unknown reason you try to act more awake than you are. Immediately, I felt a big contrac- tion that grabbed me before I’d even left the bed. I tried to find my rhythm there again, but it was not as easy or pleasant. The spell was broken. I tried the birth pool, but I didn’t feel dreamy and content. It was harder now. I felt very alert. A catch in my breath and I was floored by the pain. I remember saying “I don’t know where I am,” meaning I had lost my thread, that sense of “having the finger on the button” that had carried me through the early part of the labor. Now it felt not so much that I was having labor but that labor was having me. I was being taken over, I was roaring until I was hoarse but the pain was still more than I could express. I felt “the big stretch” that I had read about, but not registered in my last birth. I felt extreme pain in my lower back. But still there was no sign of the head. In a pause between contractions, I gave myself an internal pep talk:
“I don’t want to feel this pain anymore and there is only one way out of it: forward. Are you holding back? Are you scared? These contractions are going to keep on happening unless you go with them to the end. You need to push with everything you have got, and then this will be over. Are you scared you will break? It’s fine. They will stitch you up. They will take you to the hospital to put you back together again if that is what it takes. You are not going to die from this. It is time to let go and end it.”
The contraction started and I pushed. “There’s the head,” I said, hoping I’d catch my own baby this time. Another push. “And there’s the body,” I said as I felt it slide past my hand behind me, towards my partner Ed. The midwife told him to pick up the baby, and the touch of concern in her voice was enough to trigger all my adrenalin-soaked hyper-worry. I hurried to lift the baby from his hands and out of the water and into my arms. He was perfect, wonderful. We retired to our big yellow sofa and watched in amazement as he did the “birth crawl” up my chest to latch on himself for his first feed.
Rachele later told me that my contractions never took on the kind of consistency or length that would have been considered an established labor by a hospital. If I’d chosen a hospital birth, I would likely have been given synthetic oxytocin again. As it was, with my home birth, the love, respect, privacy, familiarity, and support enabled a journey that was pleasurable (at times), profound (throughout) and intricately suited for my particular needs. Looking back, I was struck by how very different my own experiences of birth had been to my grandmother’s. I felt profoundly grateful for all those influences that had gifted me the chance to make the choices I did: anthropologists like Robbie Davis-Floyd and Sheila Kitzinger, and activists like my mother and my midwives.
VIII
What would a social theory of birth as possibilities look like? Graeber was a social theorist. But he was also a meta-theorist. He attempted to rethink what social theory could be. One role he saw for social theory was to:
look at those who are creating viable alternatives, try to figure out what might be the larger implications of what they are (already) doing, and then offer those ideas back, not as prescriptions, but as contributions, possibilities—as gifts.
He also identified another method:
start out from some aspect … that seems particularly bleak, depressing … some failure, stumbling block … and try to recuperate something, some hidden aspect we usually don’t notice, some angle from which the same apparently desolate landscape might look entirely different.
We might think of these as two paths that both lead toward social theory as possibility.
Birthing possibilities, then, would include recuperating something from the apparently desolate landscape that confronts birth today. In Australia, at least one in three women who give birth experience birth trauma. One in ten develop signs of post-traumatic stress. People rarely speak plainly of birth, and even more rarely spell out the details in positive terms. When I have spoken in public forums about birth, including the materials that I have shared above, it is usual for at least a couple of people in the audience to use the question time to share their own birth traumas, or even to speak of traumatic births that they have only seen depicted in Hollywood movies, as a critique of my presentation of birth as possibility: it is almost if they want to say “What right do you have to speak of births so positively—your own or anyone’s—when there is so much trauma in birth?”
This trauma is real. And this trauma is cultural. Birth is, in anthropological parlance, “biocultural.” Cultural meanings and physiological processes are mutually entangled in feedback loops. For instance, people approaching their first birth who have received cultural messaging about birth as trauma, perhaps through the rituals of worry that are so common during pregnancy, or perhaps through the Hollywood movies that dwell on birth trauma, may then be predisposed during labor to pull the trigger on the “cascade of interventions,” one leading to the next. This stream of inter- ventions may itself be traumatizing and perhaps life-threatening. If so, these are more likely to be spoken of and easily heard, because they are affirmed by a surrounding cultural context that already frames birth as dangerous and traumatic. Yet the statistics suggest that birth does not have to be a horror show. In Australia, women on average have a 60 percent chance of undergoing an episiotomy or caesarean section, while those who plan a home birth experience these at a rate of less than six percent. Yet less than 1 percent of women who give birth in Australia plan a home birth. More women give birth on the side of the road each year. There are possibilities for better births.
A small but determined and wonderfully committed Australian birth activism scene is campaigning for continuity of care for women who birth in hospital, and for access to home birth for women who want it. A social theory of birthing possibilities would include offering back to birth activists some reflections on the larger implications of what they are doing. Graeber included hospitals among his list of “the very machinery of alienation.” He described these as the:
instruments through which the human imagination is smashed and shattered. Insurrectionary moments occur when this bureaucratic apparatus is neutralized. Doing so always seems to have the effect of throwing horizons of possibility wide open. This is only to be expected if one of the main things that apparatus normally does is to enforce extremely limited ones.
By keeping open the possibility of birth outside hospitals, birth activists may (intentionally or not) be throwing open much wider horizons of possibility. One area where birth activism and the anthropology of David Graeber already overlap is in an interest in the medieval history of Europe. For birth activists, the inspiration here is often the midwife (the “with- woman”), who had a high status in medieval times but, with the rise of possessive individualism, increasingly became associated with witchcraft, filth, and superstition. Another genealogy that birth activists trace back to medieval times is to the “godsibs” (or gossips): the female friends and relatives who gathered around a woman lying-in during and after birth for talk, festivities, and companionship. At a lying-in, the patriarchal hierarchy of the household and wider society was temporarily inverted, placing “women on top.” Over time, however, the rituals of lying-in became associated with mere idle “gossip and tittle-tattle.” By the mid-eighteenth century, the word “gossip” had approached its current usage, so that Samuel Johnson could define a gossip as “One who runs about tattling like women at a lying in.” Here, I wish to contribute to this line of thinking in birth activism by connecting it to David Graeber’s anthropology, particularly by way of Mikhail Bakhtin.
Bakhtin’s analysis of François Rabelais’ novels was a key inspiration for Graeber’s account of manners and hierarchy in his 2007 Possibilities. Bakhtin argued that Rabelais’ novels were popular in the Renaissance partly because they were written in a genre drawn directly from the folk culture of medieval Europe, what he calls “the language of the marketplace.” This humorous and exaggerated style thrived alongside and despite the otherwise very serious tone of medieval ecclesiastical and feudal culture. It continued into the Renaissance, proving to be a fertile source not only of relief, but also for thinking about renewal, and about the changes, even “revolution” taking place during the Renaissance. Medieval towns such as Lyon, he said, would spend as much as two months a year in a state of carnival, a state Bakhtin defines as comic, playful, and sensuous. This was a folk culture of clowns and fools, but by no means trivial. It was one half of the “double aspect” of medieval culture, a contrasting but profound pair to the austere protocols and rituals of church and state. Over time, however, carnival became more constrained and retreated to private settings. Feasts, for instance, shifted from town-wide events to brief, private affairs now mostly experienced at home. The medieval period came to be thought of in terms of gothic austerity, and the laughing nature of much popular experience of that era was all but forgotten. Readers coming to Rabelais in later times thus found themselves bewildered, and strained to find meaning in his billingsgate, blazons and parodies. Bahktin identified Rabelais’ style, and the style of the folk culture that inspired it, as “carnivalesque.” Carnival forms and symbols, he argued, signaled a temporary liberation from existing rank and order, and were always found in “(m)oments of death and revival, of change and renewal.”
Bakhtin is not often thought of as a contributor to theorizations of birth or gender, but he often evokes birth in his attempt to describe and define the carnivalesque. Birth even appears in Bakhtin’s writings a kind of master metaphor for the concept of the carnivalesque as a whole: he wrote of carnival as the “maternal womb” for the all-people through which the old would die and the new could be born. Birth is one of the bodily func- tions that is physically located on “the lower stratum” that was the typical focal point of carnival symbolism. In carnival culture, the lower areas of the body, especially the female body, were a common source of humor and “degradation.” But in carnival degradation was understood as a form of coming down to earth, an earth which was at once both the grave and the womb. The lower stratum was returned to as a source of renewal, even as it was also a source of decay and death. Birth and death were often linked in carnivalesque imagery (such as birth-giving deaths, or death-giving births), an imagery that dwelt overwhelmingly on the openings and pro- trusions of the body—eating, bellies, defecation, and so on—an imagery that Bahktin called “grotesque realism.” He described the lower stratum as “the fruitful earth and the womb. It is always conceiving.”
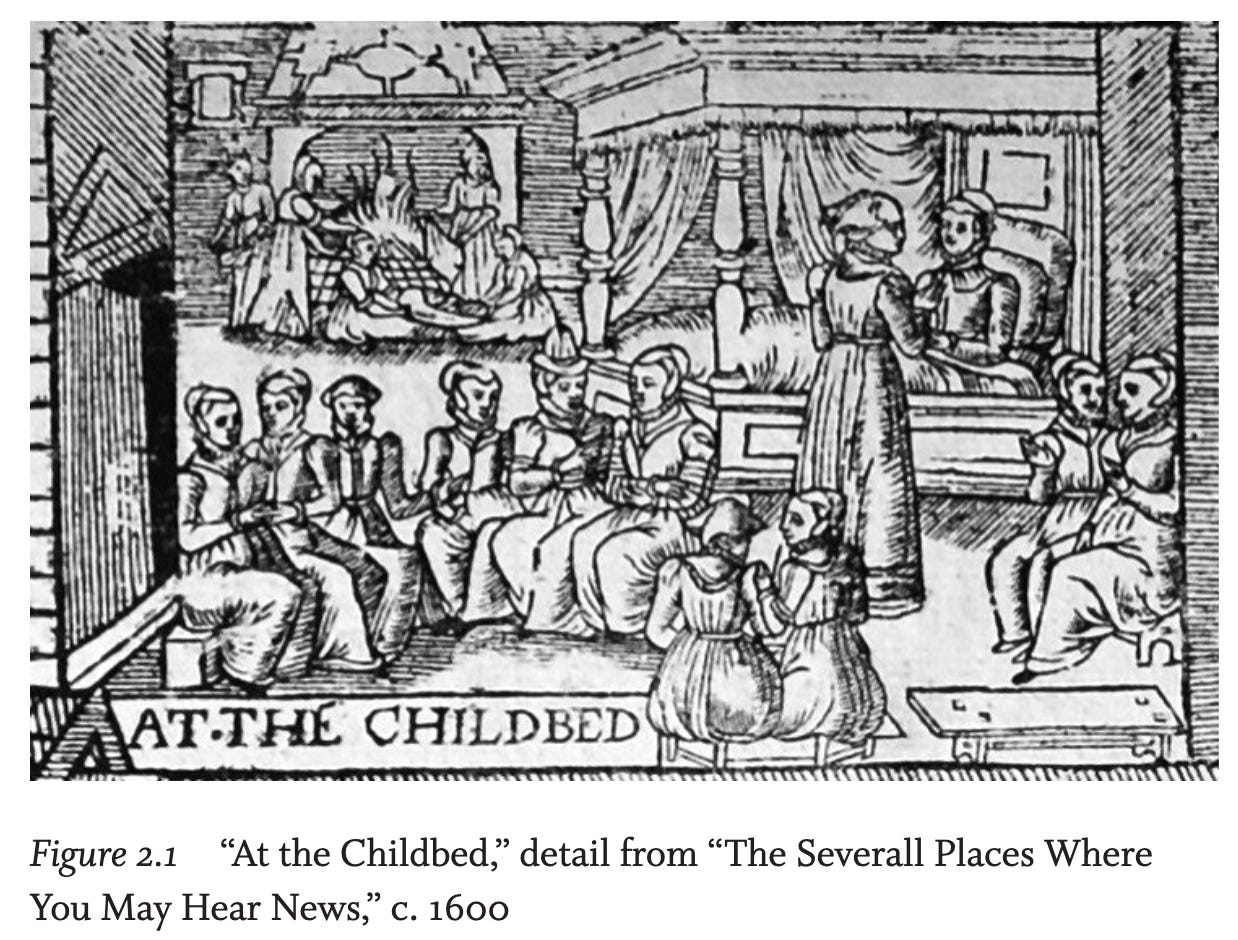
In medieval Europe, grotesque realism had a deeply positive connotation: it was the base stratum which united all people and indeed all the cosmos. Yet, over time, these images and symbols shifted in meaning, so that today these self-same bodily features and processes are at best con- sidered private, trivial and severed from other spheres of life, or at worst as carrying only negative connotations. One of the examples Bakhtin gives of this shift is the revolution that took place in the ritual and sym- bolism of birth. He discusses the Caquet de l’accouchée (“The Cackle of the Confined Woman”), a broadsheet first published in France sometime in 1560. The pamphlet was apparently quite popular, and was republished in varied editions in both Europe and England. Bakhtin explains that, at the time these were published, it was usual for women and girls to continue lying-ins. These were characteristically carnivalesque, with a suspension of social conventions, ample food, and frank conversation, especially about “the material bodily lower stratum.” In the “Cackle,” however, this old tradition was represented as shallow and meaningless, as merely one of the “severall places where you may hear news”. Bakhtin understood this shift as part of a historical process whereby the carnivalesque unity of birth and death, which had affirmed the cosmic importance of bodily processes, especially those of the lower stratum, was being sundered, leaving each holding only a rather negative meaning: their continued association with defecation and urination (other “lower stratum” elements) rendered birth and postpartum now as trivial, private, and faintly embarrassing. This, he maintained, is the contemporary meaning attached to birth.
Inspired by Bahktin’s account, Graeber analyzed the shift in manners during this period arguing that, “Basic standards of how one was expected to eat, drink, sleep, excrete, make love, shifted almost completely.” Graeber argued that the decline in medieval carnivalesque was associated with the rise of possessive individualism that valued “avoidance” relations, as evidenced in bodies that presented themselves as closed-off and contained. He drew on C.B. MacPherson’s argument that possessive individualism, evident in liberal-democratic theory from the seventeenth century through to contemporary times, assumes that one holds autonomy over one’s own “person or capacities, owing nothing to society for them.” Graeber argued that this implicit philosophy guided not only dominant political and economic theories, but also the most intimate interactions of daily life, including common courtesies. Graeber argued that as the carnivalesque vernacular became more and more muted, if not forgot- ten altogether, it was displaced by an understanding of the body as the prime possession of an individual who owed nothing to anyone. Orifices, which betrayed this sense of the enclosed self by opening up to the other, were hidden from view and became a private matter. Eating, drinking, sexual life, and defecation became individual matters with narrow, trivial, and domestic connotations, “torn away from direct relation to the life of society and to the cosmic whole.” This shift is discernible in sentiments around birth, too: the gossip moved from her place at the lying-in to the place of a small-minded tattler of private tales. And birth, too, moved from the bawdiness of the lying-in to the closed-off world of avoidance so aptly embodied by the hospital.
Today—with the pervasive cultural influence of possessive individualism—sexuality, birth, and breastfeeding are uncomfortable reminders that, in fact: “we are not discrete beings; we emerge from other people, we merge into other people, our lives leak literally and figuratively into one another […].” With birth, one might speak of a possessed individ- ual, rather than a possessive one. The pregnant woman has another within her. Insofar as a pregnant woman is able to make choices around birth and pregnancy, these are choices about if and how to make room “for the Other in her own way of being.” Birth activists’ campaigns for continuity of care—where a woman planning to birth at hospital could expect a stable team throughout her antenatal and postnatal care, and the right to a home birth if she so chooses—challenge possessive individualism and the rituals of avoidance that sustain it. The hospital promises bright lights, distant professionals, clean surfaces, and sterile tools. Visiting hours and numbers are limited. Birth is set apart from the day-to-day world: a potentially abstract space. As Robbie Davis-Floyd notes, most North American women—indeed, women all over the world, especially those in high-resource countries— seek out such spaces for birth. Part of the appeal, I suspect, arises from today’s societal discomfort with and denigration of the lower stratum, orifices, and leakages. Hospitals appeal because they offer an abstract space where bodies can be imagined through relations of avoidance, even in the extremes presented by birth. This is particularly clear in many Australian women’s aspiration to have an obstetrician attend their births: a stranger who they will most likely barely know, but one of high status. The continuity-of-care model, by contrast, offers women not abstraction but familiarity and community. And the home birth offers women a birth tangled in with the comings and goings of everyday life: an inversion of the day-to-day, but not an avoidance of it. One of the larger implications of birth activism, then, is the challenge it presents to the cultural normalization of possessive individualism. Possessive individualism predisposes us to forget our continuity with each other, with the land, with the dead, and with the generations yet to come, even when our bodily experiences suggest otherwise. The need to move beyond such ways of thinking is now urgent and is a matter of survival for our own species and many others. Birth continues to be an important rite of passage. This means that in births, cultural meanings are transmitted but can also, possibly, be transformed.
Birth activism, the choices women make in planning their births, and those who work to support them in those choices, have profound importance, not only for the individuals involved but also for the possibilities of social change and for the future of humanity more broadly. Like the witches imagined by Ehrenreich and English, birth activists today hold out “the hope of change in this world.” A final note is necessary here on the idea of birth choices. The idea of a choice-making individual is core to possessive individualism: a person is conceived of as the rightful possessor of their body as if it were one of their belongings. In her 1988 Gender of the Gift, Marilyn Strathern noted that dominant strains of Western feminism have tended to reproduce this concept of the body, defining gender justice importantly in terms of women’s ownership of their own bodies. One of the contradictions of birth activism is that so much of it is framed in terms of defending birthing women’s abilities to make choices about their bodies, yet a woman at the alter/altar of birth has an opportunity to experience herself precisely as overcome by a force that might temporarily displace her rational, decision-making self: as possessed rather than possessive. At the same time, it is often noted that the more first-time parents plan their births, seemingly the more things go awry. The more we see birthing as something to plan and make informed choices about, the more rates of intervention rise. There is something uncomfortable, then, in defining the goals of birth activism in terms of choices.
One possible way of thinking about this apparent contradiction is in terms of the kinds of choices that are actually at stake. Birth choices are not like the choices made by, say, an architect planning a building. Nor are they like the choices made by an individual who owes nothing to anyone and thinks only of their own self-interest or profit. They are cer- tainly not like the choices made about one’s possessions. Ideally, birth choices would instead be more akin to the choices made by free people. By this, I mean freedom in Graeber’s sense: not freedom from obligations, but freedom to choose one’s obligations and to live only under those constraints. For Graeber, “The revolution begins by asking: what sort of promises do free men and women make to one another, and how, by making them, do we begin to make another world?” He noted that we barely have any experience of being free in this way. We do not live in a free society. We can only work towards making one a possibility. Even so, Graeber reminds us that we can, in the here and now, insist on living as if we were already free. Birth choices that insist on this kind of freedom have implications not only for satisfaction among new parents, but also for more expansive imaginations of the possibilities for ourselves and our place in the world.
Notes
1. David Graeber, The Democracy Project: A History, a Crisis, a Movement
(New York: Spiegel & Grau, 2013), 237.
2. Henrietta Moore, A Passion for Difference: Essays in Anthropology and
Gender (Cambridge: Polity Press, 1994).
3. Robbie E. Davis-Floyd, “The Rituals of American Hospital Birth,” in Con-
formity and Conflict: Readings in Cultural Anthropology, ed. David McCurdy
(New York: HarperCollins, 1996).
4. Arnold van Gennep, The Rites of Passage (London: Routledge & Kegan
Paul, 1960).
5. Victor Turner, The Ritual Process: Structure and Anti-Structure (New York:
Aldine De Gruyter, 1969).
6. I use jam here in the sense of “culture jamming,” a method of using widely
recognized social symbols in a way that upturn or reverse their meaning.
7. Davis-Floyd, “The Rituals of American Hospital Birth.”
8. Michel Odent, The Functions of the Orgasms: The Highways to Transcen-
dence (London: Pinter and Martin, 2009).
9. Charles H.P. Zuckerman, “Good Gambling: Meaning and Moral Economy
in Late-Socialist Laos” (PhD diss., University of Michigan, 2018).
10. David Graeber, Direct Action: An Ethnography (Oakland, CA and Edin-
burgh: AK Press, 2009), x.
11. Faye D. Ginsburg and Rayna Rapp, Conceiving the New World Order: The
Global Politics of Reproduction (Berkeley: University of California Press,
1995). This is the book that, by popular consensus among reproductive
scholars, officially founded the anthropology of reproduction.
12. Suzie Hayman, “Sheila Kitzinger Obituary: Author and Pioneer of Natural
Childbirth who Led a Crusade against its Medicalisation,” The Guardian,
April 13, 2015, https://www.theguardian.com/lifeandstyle/2015/apr/12/
sheila-kitzinger (accessed May 20, 2021).
13. Sheila Kitzinger, The New Experience of Childbirth (London: Orion, 2004).
14. Sheila Kitzinger, “The Great Childbirth Blackmail,” Daily Mail, June 14,
2001.
15. Sheila Kitzinger, “Birth as a Rape: There Must Be an End to ‘Just in Case’
Obstetrics,” British Journal of Midwifery 14, no. 9 (2006).
16. I thank Robbie Davis-Floyd (pers. comm.) for this observation and
general comments.
17. Brigitte Jordan, Birth in Four Cultures: A Crosscultural Investigation of Child-
birth in Yucatan, Holland, Sweden, and the United States, 4th edn (Long
Grove, IL: Waveland Press, 1993).
18. Carol McCormack, Ethnography of Fertility and Birth, 2nd edn (Long
Grove, IL: Waveland Press, 1994).
19. Sheila Kitzinger Ourselves as Mothers: The Universal Experience of Mother-
hood (Boston, MA: Da Capo Press, 1995).
76 As If Already Free
20. I recollect one of my first anthropology lecturers, Christine Helliwell,
commenting acerbically on one of my undergraduate essays in 1994 that
“all human societies use technology.” See for instance the use of such terms
in Sheila Kitzinger, Ourselves as Mothers.
21. Ibid., 239.
22. Eleanor Burke Leacock, Myths of Male Dominance: Collected Articles on
Women Cross-Culturally (New York and London: Monthly Review Press,
1981).
23. Ginsburg and Rapp, Conceiving the New World Order, 2.
24. George W. Stocking, The Ethnographer’s Magic and Other Essays in the
History of Anthropology (Madison: University of Wisconsin Press, 1992).
25. Ibid., 363.
26. Richard A. O’Connor, “Agricultural Change and Ethnic Succession in
Southeast Asian States: A Case for Regional Anthropology,” Journal of
Asian Studies 54, no. 4 (1995): 968–996.
27. Sheila Kitzinger, Rediscovering Birth (Boston and London: Little Brown,
2000).
28. David Graeber, Fragments of an Anarchist Anthropology (Chicago: Prickly
Paradigm Press, 2004), 96. Parentheses added.
29. Graeber, Fragments, 96.
30. David Graeber, Debt: The First 5,000 Years (Brooklyn: Melville House,
2011).
31. Orli Dahan, “The Riddle of the Extreme Ends of the Birth Experience:
Birthing Consciousness and its Fragility,” Current Psychology 42, no. 1
(January 2023): 262–272.
32. Alieta Belle and Jenny Blyth, “The big stretch: Insights about birth”
(DVD) and “The big stretch: The sequel” (DVD). N.D. Birthwork.
33. Graeber, Fragments, 12.
34. David Graeber, Revolutions in Reverse: Essays on Politics, Violence, Art, and
Imagination (London and New York: Minor Compositions, 2011), 4.
35. Paige L. Tsakmakis, Shahinnoor Akter, and Meghan A. Bohren, “A Qual-
itative Exploration of Women’s and their Partners’ Experiences of Birth
Trauma in Australia, Utilising Critical Feminist Theory,” Women and
Birth: Journal of the Australian College of Midwives epub ahead of print
(December 24, 2022), doi 10.1016/j.wombi.2022.12.004.
36. Clara-Sophie Heyne, Maria Kazmierczak, Ronnie Souday, Danny Horesh,
Mijke Lambregtse-van den Berg, Tobias Weigl et al., “Prevalence and Risk
Factors of Birth-Related Posttraumatic Stress among Parents: A Compar-
ative Systematic Review and Meta-Analysis,” Clinical Psychology Review 94
(June 2022): 102157.
37. Davis-Floyd, “The Rituals of American Hospital Birth.”
38. Australian Institute of Health and Welfare, “Australia’s Mothers and
Babies, Summary,” December 14, 2022, available at: https://www.aihw.
gov.au/reports/mothers-babies/australias-mothers-babies/contents/
summary (accessed April 17, 2023).
Birthing Possibilities 77
39. Miranda L. Davies-Tuck, Euan M. Wallace, Mary-Ann Davey, Vickie
Veitch, and Jeremy Oats, “Planned Private Homebirth in Victoria 2000–
2015: A Retrospective Cohort Study of Victorian Perinatal Data,” BMC
Pregnancy and Childbirth 18, no. 1 (September 1, 2018): 1–8.
40. Hazel Keedle, Virginia Schmied, Elaine Burns, and Hannah G. Dahlen,
“Women’s Reasons for, and Experiences of, Choosing a Homebirth Fol-
lowing a Caesarean Section,” BMC Pregnancy & Childbirth 15, no. 1
(September 4, 2015): 1–12.
41. Australian Institute of Health and Welfare, “Australia’s Mothers and
Babies: Place of Birth,” available at: https://www.aihw.gov.au/reports/
mothers-babies/australias-mothers-babies/contents/labour-and-birth/
place-of-birth (accessed March 21, 2023).
42. Graeber, Revolutions in Reverse, 60.
43. See for instance the classic pamphlet published by Barbara Ehrenreich
and Deirdre English in 1973, “Witches, Midwives and Nurses: A History
of Women Healers” (Feminist Press, CUNY), reprinted as a book in 2010:
Barbara Ehrenreich and Deirdre English, Witches, Midwives, and Nurses: A
History of Women Healers (New York: The Feminist Press, 2010).
44. Adrian Wilson, “The Ceremony of Birth and its Interpretation,” in Women
as Mothers in Pre-Industrial England: Essays in Memory of Dorothy McLaren,
ed. Valerie Fildes (London and New York: Routledge, 2013), 93.
45. Mikhail Bakhtin, Rabelais and his World, trans. Helene Iswolsky (Bloom-
ington: Indiana University Press, 1984), 105.
46. Quoted in Gail McMurray Gibson, “Scene and Obscene: Seeing and Per-
formance in Medieval Childbirth,” Journal of Medieval and Early Modern
Studies 29, no.1 (1999), 11.
47. David Graeber, “Manners, Deference, and Private Property: Or, Elements
for a General Theory of Hierarchy,” in Possibilities: Essays on Hierarchy,
Rebellion, and Desire (Oakland, CA and Edinburgh: AK Press, 2007),
13–56.
48. Bakhtin, Rabelais and his World, 9.
49. Ibid., 21.
50. Ibid., 21.
51. See Megan Marie Inbody, “Town/Gown Relations: The Forms and Func-
tions of Female Gossip Communities and Networks in Early Modern
Comedy” (PhD diss., Michigan State University, English, 2012), 203.
52. The examples Bahktin draws on were pamphlets published in 1622 and
1663 (Bakhtin, Rabelais and his World, 106); the example pictured in
Figure 2.1 is from 1600 (Inbody, “Town/Gown Relations,” 203).
53. Bakhtin, Rabelais and his World, 105.
54. Graeber, Possibilities, 14.
55. Crawford Braugh MacPherson, The Political Theory of Possessive Individ-
ualism: Hobbes to Locke (Oxford and New York: Oxford University Press,
1962), 3.
56. Bakhtin, Rabelais and his World, 321.
78 As If Already Free
57. Penny van Esterik and Richard A. O’Connor, The Dance of Nurture: Nego-
tiating Infant Feeding (New York and Oxford: Berghahn, 2017), 16.
58. Kalpana Ram, Fertile Disorder: Spirit Possession and its Provocation of the
Modern (Honolulu: University of Hawai’i Press, 2013), 144.
59. Davis-Floyd, “The Rituals of American Hospital Birth.”
60. Ibid., 14.
61. Marilyn Strathern, The Gender of the Gift: Problems with Women and
Problems with Society in Melanesia (Berkeley: University of California
Press, 1988).
62. Tina Miller, “‘We’ve Bought a Tens Machine and We’re Trying Aromather-
apy and Hypnobirthing’: Being Prepared for Labour and Birth?” Studies in
the Maternal 13, no. 1 (2020).
63. Graeber, Revolutions in Reverse, 39
"Of all countries in 2020, the United States possessed the highest infant mortality rate at 5.4 deaths per 1000 live births, which is markedly higher than the 1.6 deaths per 1000 live births in Norway, which has the the lowest mortality rate."
https://www.ajmc.com/view/us-has-highest-infant-maternal-mortality-rates-despite-the-most-health-care-spending
"More women are having children later in life and more women are entering pregnancy with chronic conditions such as hypertension, obesity, diabetes, and cardiovascular disease. The rising number of Cesarean sections – a major surgery that is not always necessary – is also believed to be a contributor."
One should ask why so many young women suffer from life threatening chronic conditions. Does it have something to do with pharmaceuticals, vaccines, or the chemicals inundating the food supply.
And what is it about the culture that's causing women to defer childbirth to their late 30's or early 40's.
As far as "C sections" are concerned they're more medically profitable as well as expedient since the delivery can be planned down to the minute. Unfortunately, it results in a longer recovery for the mother.
"Most people stay in the hospital between two and three days. A full recovery can take between four and six weeks. Most providers recommend avoiding steps, lifting, exercise and other strenuous activities for several weeks."
https://my.clevelandclinic.org/health/treatments/7246-cesarean-birth-c-section
Caesarean Section was/is applied because:
STATE interference when
- the mother was dead or dying, as an attempt to save the child for a state wishing to increase its population,
MEDICAL reasons when
- baby is positioned bottom or feet first (breech) and can't be turned,
- cervix (opening to the womb) is blocked by the placenta (placenta praevia),
- baby is lying sideways (transverse) and can't be turned by the doctor,
DIRECT MONETARY reasons because
- a Caesarean Section is more profitable for the hospital and professionals involved,
- can be planned to the minute (don't you dare ruining my weekend ...!!),
INTERCOURSE reasons
- female genital anatomy is unaltered by birth-giving, hence "same feel" ... and last-not-least
INDIRECT MONETARY reasons because
- Caesarean Section prevents the foetus from being imbibed with the micro-biome specific to the mother's vaginal environment, hence impeding the newborn's immune-system being primed for a life on a planet where bacteria and numerous pathogens are dominant.
It is obvious that BIG PHARMA silently promotes Caesarian Section, securing them millions of life-long patients and perfectly fraudulent, but legal wind-fall profits !!